Description

Copyright infringement not intended
Context: The Rajasthan Assembly's recently completed budget session restarted discussion about the Right to Health Bill.
Details
- If the bill is approved, hospitals, clinics, and laboratories that are both publicly and privately operated must offer free and reasonably priced medical services.
- The Bill is opposed by private hospital doctors who claim it was quickly drafted, ignores practical considerations, and could tighten standards in an industry that is already overly regulated.
.jpeg)
Key points of the Bill
- The Right to Healthcare Bill, 2022 was introduced to the State Legislature by the Rajasthan State government in September 2022. Patients and healthcare professionals are given rights under the Bill, which also obliges the government to uphold these legal rights and requires the establishment of grievance redressal systems.
- Residents of Rajasthan will be entitled to free examinations, medications, diagnostics, emergency transport, and care at all public health facilities, as well as reasonably priced surgeries. The Bill views healthcare as a public good rather than as a means of profit.
- 20 rights are outlined in clause 3 of the bill, including the right to informed consent, the right to information (in the form of medical records and documentation) regarding diagnosis and treatment, and the right to treatment free from caste, class, age, gender, and other discrimination.
- The obligation for providing adequate medical services is transferred to the government under Section 4 of the Bill. The government is "obligated" to allocate funding, establish institutions, and create grievance redressal procedures.
- The government must create a human resource policy for the health sector under section 4, which calls for a fair distribution of physicians, nurses, and other healthcare professionals throughout all levels of the system.
Concern
- Due to the lack of clarity over who will be responsible for paying for the required free emergency treatment, private healthcare providers have been the most vocal opponents of the Bill.
- After protests, the government decided to establish a fund to pay for any emergency medical services provided by the private sector.
- Critics claim that it is an attempt to surrender the State's duty to provide health protection and increases the burden of patients on the private sector.
- Many believe that the Bill is unnecessary and highly restrictive.
- The Bill contains the word "guarantee" just in passing, and there is no mention of a deadline for formulating the guidelines, which leaves room for interpretation over when an Act will be put into effect.
|
Right to health under the Indian Constitution
● The right to health is not specifically mentioned in the Indian Constitution. The theoretical "right to health" is drawn from the constitutionally protected rights to life and liberty (Article 21).
● In the past, courts have underlined the State's duty to safeguard and advance citizens' health, citing constitutional clauses like Article 38 (promotes the welfare of people) and Article 47 (directs the government to meet the population's nutritional and health needs).
|

State of India’s healthcare sector
- India had 7 physicians per 1,00,000 people in 2017 (in contrast to 98 in Pakistan, 100 in Sri Lanka and 241 in Japan).
- 53 beds per 1,00,000 people(in contrast to 63 in Pakistan, 79.5 in Bangladesh, 415 in Sri Lanka and 1,298 in Japan).
- 7 nurses and midwives per 1,00,000 people(in contrast to 220 in Sri Lanka, 40 in Bangladesh, 70 in Pakistan, and 1,220 in Japan).
- India has among the highest out-of-pocket (OOP) expenditures of all countries in the world- 62% of the total health expenditure in India is OOP.
How much does India spend on healthcare?
- In 2020-21, India spent 1.8% of its gross domestic product (GDP) on healthcare.
- With ‘health and well-being one of the six pillars of the Union Budget 2021-22, the government has committed approximately 2.5-3% of GDP now.
- Data shows that India has 1.4 beds per 1,000 people, 1 doctor per 1,445 people, and 1.7 nurses per 1,000 people.
- According to the World Health Organization (WHO), India ranks 184 out of 191 countries in health spending.
- The US spends over 16% of its total GDP on healthcare, while Japan, Canada, Germany etc. spend over 10% of their GDP on healthcare.
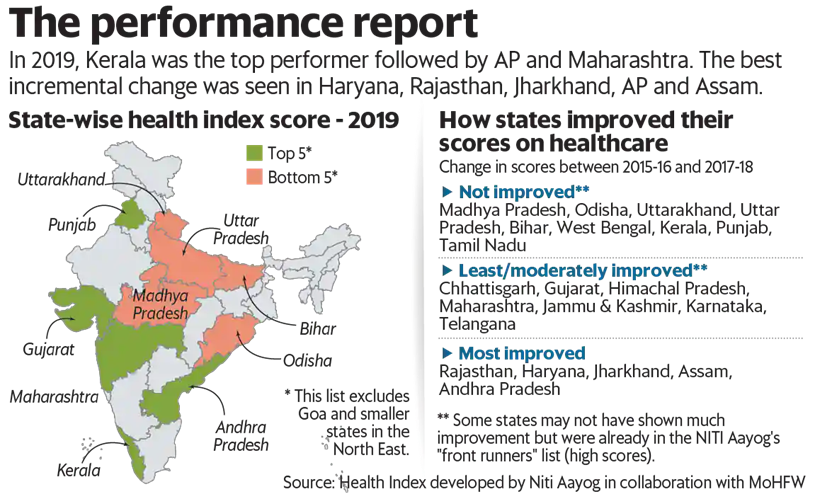
How do states rank on the health index?
- The Health Index for States developed by Niti Aayog in consultation with the health ministry and the World Bank has rankings for large states, smaller states and Union territories.
- It is based on 23 health parameters ranging from mortality rate and sex ratio to functioning cardiac care units.
- In 2019, Kerala was the top performer followed by Andhra Pradesh and Maharashtra.
- The index results indicated that states even with a lower economic output are performing better on health and well-being.
Problems with Health Care Infrastructure of India:
Shortage of Staff and Equipment
- The government Rural Health Survey reveals that only 55.6% of CHCs have functional X-ray machines while only 18% of the specialists required are in place.
- Overall there was a shortfall of 86.5% surgeons; 74.1% obstetricians &gynaecologists; 84.6% general physicians and 81% paediatricians at CHCs in the country.
- According to Rural Health Statistics 2018 only 8% of subcentres, 12% PHCs and 13% CHCs met Indian Public Health Standards.
- Healthcare infrastructure is heavily skewed in favour of urban areas
- The evidence shows that the private healthcare market occupies a large share of hospitals (75%), hospital beds (50.7%) and medical institutions (54.3%) largely located in urban areas.
- Almost half (48%) of the large private hospitals and two-thirds of corporate hospitals are located in five million plus cities in India.
- Around 80% work in urban areas while 69% of rural India is heavily dependent on the public health system where the allopathic doctor population ratio is 1:11,082 while the World Health Organization recommends a ratio of 1:1000.
Inter-State and Intra-state variations
- In a few states such as Kerala, Tamil Nadu and Delhi public health facilities play their intended role of being the first point of care and proactively delivering essential services while in some states like Uttar Pradesh, Bihar, and Jharkhand primary health care is not available to masses and they are highly dependent on the private sector with their expenditure.
- While the private facility is highly urban-centric covering a few districts of India, there is a dearth of both public and private health care facilities in many of the districts and there are many parts/areas/districts where no one is to serve people.
No proper regulatory mechanism and monitoring
- According to a WHO report published in 2016, Only one in five doctors in rural India is qualified to practice medicine.
- The report said that 31.4% of those calling themselves allopathic doctors were educated only up to class 12 and 57.3% of doctors did not have a medical qualification.
- Due to poor regulatory mechanisms and monitoring, private health care services and doctors are following unethical, greedy practices treating medical services as a business and hospitalisation as a source of profit, writing unnecessary diagnostic tests, high-rate medicines instead of generic ones, organ theft (kidney racket) etc. even denying treatment to poor people though getting land from the government on a subsidised rate.
Lack of Affordability:
- The contribution of the private sector to healthcare expenditure in India is around 80 per cent while the rest 20 per cent is contributed by the Public Sector.
- The private sector also provides for 58 per cent of the hospitals and 81 per cent of the doctors in India.
Way forward:
- Primary health Centres need to be strengthened as 80-90% health needs of a person in a lifetime can be provided by primary health care centres. For this, in urban areas, Mohalla clinics can be a good alternative while in villages SCs and PHCs should be strengthened.
- Increase the expenditure on health to 2.5% as envisaged in NHP 2017 to improve infrastructure in health centres.
- To meet the shortage and availability of trained staff at PHCs and CHCs preference should be given to local people. Skills of good performing ASHA, ANM workers and nurses should be upgraded and they should be posted in their own rural and remote areas of PHCs and CHCs.
- To remove misallocation, new medical colleges whether it is private or public should be opened strictly only in rural and remote areas. Special focus should be on large populous northern states or backward states.
- There should be proper regulation and monitoring against all the malpractices prevalent in a health area. Stringent laws and punishment should be there for all those who do unethical practices in this field.
- The use of technology can help a lot to reduce costs as well as improve facilities in a health area.
- Overall help of community people should be sought for providing health care to all because no programme can be successful without the active involvement of the community. Kerala is a good example of it that took the help of educated youth and Panchayati Raj Institutions for implementing her health programmes.
- A National Health Regulatory and Development Framework needs to be made for improving the quality (for example registration of health practitioners), performance, equity, efficacy and accountability of healthcare delivery across the country.
- Increase the Public-Private Partnership to increase the last-mile reach of healthcare.
- Generic drugs and Jan Aushadi Kendras should be increased to make medicines affordable and reduce the major component of Out of Pocket Expenditure.
- The government’s National Innovation Council, should encourage a culture of innovation in India and help develop policy on innovations that will focus on an Indian model for inclusive growth.
- India should learn from other developing countries like Thailand to work towards providing Universal Health Coverage.UHC includes three components: Population coverage, disease coverage and cost coverage.
|
PRACTICE QUESTION
Q. Examine the issues that the Indian healthcare system is experiencing and make suggestions to raise the standard and accessibility of healthcare in the nation.
|
https://epaper.thehindu.com/ccidist-ws/th/th_delhi/issues/28379/OPS/G3NAVTQ8P.1.png?cropFromPage=true









.jpg)
{kind=link}